 That graph up there shows the main outcomes of the AGE Trial, a large study of mammography screening in England that asked the question “Does offering mammograms to women in their 40’s save lives?” The dotted red line represents the mortality from breast cancer in women offered mammograms annually between ages 40 and 48 through the National Health Service (or NHS). The solid line represents the control group of women who were not offered mammogram screening by the NHS until after age 50.
That graph up there shows the main outcomes of the AGE Trial, a large study of mammography screening in England that asked the question “Does offering mammograms to women in their 40’s save lives?” The dotted red line represents the mortality from breast cancer in women offered mammograms annually between ages 40 and 48 through the National Health Service (or NHS). The solid line represents the control group of women who were not offered mammogram screening by the NHS until after age 50.
The investigators are interpreting that graph to mean that mammograms in women under age 50 are not worth doing.
Let’s talk, shall we?
The study, which was published Dec 9 in the Lancet, randomized 160,921 women on a 1:2 basis to either annual mamograms from age 40-48 or to a control group of “usual care”, which in the NHS is an invitation to a first mammogram between ages 50-52. Deaths were identified through the NHS central registry for a mean follow up of 10.7 years.
There was a 17% reduction in breast cancer mortality in the early screen group. (That’s the graph up there)
As it turns out, only 69% of the women invited to screen actually came for the initial screening, and overall, only 81% of them ever got a mammogram during the study. The women who never showed up for the mammograms had a higher rate of breast cancer deaths than those who got the screening. When adjusting for these two factors, the investigators found that women who actually showed up for the early mammograms had a 24% reduction in mortality from breast cancer compared with the control group.
Sounds pretty clear, doesn’t it?
Well, unfortunately, it’s not. You see, neither the numbers I quoted nor the difference up there in the graph between the red and black lines is statistically significant.
Why not? Very possibly because the study wasn’t big enough to detect the difference in breast cancer mortality with enough certainty to call it real . You see, the NHS ran out of money and personnel partway throught the study, so the sample size was smaller than initially planned. Secondly, mortality in the control group was much lower than initially estimated, making it even harder to find a statistically significant difference with the smaller sample size. Here’s what the investigators said about this:
The power of the trial to show a reduction was diminished both by the smaller than planned sample size and by the lower than anticipated mortality from breast cancer in the control group (2·35 per 1000 vs 3·3 per 1000), resulting in a revised power of 60% to detect a 20% mortality reduction, and the CI does not exclude a reduction of 34% or an increase of 4%.
Most studies are powered at 80%, meaning that, going into the study, there is an 80% possibility that the study has enough subjects to be able to detect a difference with 95% certainty between the groups. (or something like that – statisticians, feel free to correct me.). If the study is too small, then the odds are stacked from the get-go against finding anything to hang your hat on in terms of results. And that’s what happened here.
Finally, the mammograms performed in this study were below standard. Although the first screens were standard two view mammos, subsequent screens in the under 50 group were single view only. This was done in an attempt to diminish radiation dose, but likely resulted in lower detection rates in the screened group, since single view mammograms are less sensitive and specific than two view mammos. (Current standards in both UK and US are two view mammograms.)
The end result is that the Lancet study failed to show a benefit to mammograms before age 50. What a shame – to do all that work, and have your final study size to small to detect a difference between your two groups with any confidence.
Perhaps to ease our disappointment with their study, the investigators did make a very nice graph of the clinical trials of mammograms in women under 40 to date:
 For the lay crowd, what this graph means is that the risk of dying from breast cancer in women getting mammograms before 50 is smaller relative to those who wait till after 50. (The black boxes up there) But the 95% confidence intervals (the thin lines) of almost all of these studies crosses one, meaning that the protective effect of mamograms is still not statistically significant overall. However, I would say there is a clear trend to protection against dying in the early mammogram group, wouldn’t you? (All the black boxes except one fall below 1)
For the lay crowd, what this graph means is that the risk of dying from breast cancer in women getting mammograms before 50 is smaller relative to those who wait till after 50. (The black boxes up there) But the 95% confidence intervals (the thin lines) of almost all of these studies crosses one, meaning that the protective effect of mamograms is still not statistically significant overall. However, I would say there is a clear trend to protection against dying in the early mammogram group, wouldn’t you? (All the black boxes except one fall below 1)
What about other outcomes?
Dying or living are not the only two possible outcomes that might be affected by earlier diagnosis of breast cancer. We all know that cancers picked up earlier are more likely to be amenable to breast-conserving surgery and less likely to require chemotherapy. I don’t know about you, but if I am going to get breast cancer, I would rather have it diagnosed at a stage where I can keep my breast and avoid chemo. Also, chemo can be associated with secondary cancers years later, something a 10 year study would not pick up.
Bottom line – this study adds little to our understanding of the role of today’s mammograms in women under age 50 as practiced in the United States. For my patients, I will continue to recommend mammograms every 1-2 years beginning at age 40, and annually at age 50 and above. I advise women with dense breasts to have digital mamograms and ultrasound in addition to mammography, especially if there is a family history of breast cancer.
Hopefully, the data from this latest Lancet study will not be used by the NHS to continue to deny this same screening to women in the UK. ________________________________________________
United States Preventive Services Taskforce recommendations for mammograms
NCI statement on mammograms in women under age 50
Info on Digital Mammography from the NCI
University Of Pennsylvania’s Med Page Today critique of the Lancet Study (excellent read)
Thanks to Rachel for pointing the Lancet article out to me.
Category: Second Opinions

 Thanks to Grunt Doc for pointing folks to my post series on “How to Get Pregnant“. Despite his telling readers that the series is a poke at our medicalization of normal life, it appears that some readers still don’t get me. Because once again, I’ve gotten a chiding comment from an offended reader accusing me of being insensitive to the needs of women. Here’s what Christian wrote today:
Thanks to Grunt Doc for pointing folks to my post series on “How to Get Pregnant“. Despite his telling readers that the series is a poke at our medicalization of normal life, it appears that some readers still don’t get me. Because once again, I’ve gotten a chiding comment from an offended reader accusing me of being insensitive to the needs of women. Here’s what Christian wrote today:
 When I was 13, I went on the Dr Stillman’s Water Diet and lost 25 pounds. That same summer, my brother Al decided he needed to shape up, so he did what boys do when they want to lose a few pounds. He gave up Cheetos and started running and lifting weights.
When I was 13, I went on the Dr Stillman’s Water Diet and lost 25 pounds. That same summer, my brother Al decided he needed to shape up, so he did what boys do when they want to lose a few pounds. He gave up Cheetos and started running and lifting weights.
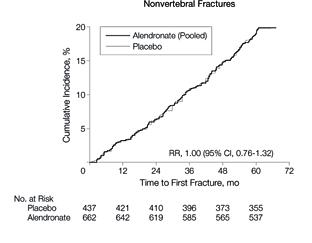 However, there was a significantly higher risk of vertebral fractures in women who stopped aledronate.
However, there was a significantly higher risk of vertebral fractures in women who stopped aledronate. 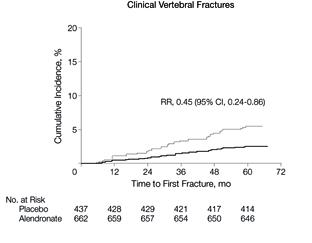







{kind=link}