See Part 1 here.
When we last left the WHI, the results of the estrogen-progesterone arm of the study had just been released. Unexpected results which showed the drug to increase the risks of heart disease, stroke and breast cancer…
The Immediate Reaction
Well, we all know what happened next.
Widespread confusion and not a little panic erupted, helped in no small part by the manner in which the WHI’s findings were released (via press release prior to publication of the paper). The investigators did little in their contact with the media to place their results in perspective or to address how they might relate to women using HRT for treatment of menopausal symptoms. Instead, they fanned the flames of hysteria by making statements to the press like “This is a dangerous drug.” (NY times) That was just irresponsible, in my opinion.
Critical analysis of the paper was lost in the melee. The fact that the WHI was never designed to study the use of HRT for treatment of menopausal symptoms was a fact that received cursory mention at most. Questions of statistical significance and relative risk were rarely mentioned. The WHI was accepted as gospel from day one. I don’t fault the media – most of the reporting I read was intelligent and well meaning. But critical analysis of the data itself was notoriously absent, because no one had time to do it before having to talk to the media.
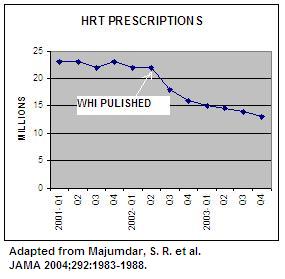
Overall, about two thirds of women who were taking HRT at the time the WHI results were released stopped their therapy; those who stayed on the drugs tended to be those women who had the worst menopausal symptoms.
 Physician reactions were just as strong. Some docs stopped prescribing HRT altogether. One doc I know told her patients, “You can kill yourself if you want to, but I am not going to prescribe the gun'”. One patient of mine was told by her former physician, “I won’t let my wife use it, and I’m not going to prescribe it for you.”
Physician reactions were just as strong. Some docs stopped prescribing HRT altogether. One doc I know told her patients, “You can kill yourself if you want to, but I am not going to prescribe the gun'”. One patient of mine was told by her former physician, “I won’t let my wife use it, and I’m not going to prescribe it for you.”
Perhaps they are worried about being sued. Given that there are more lawsuits out there against Wyeth than you can count, I can’t say as I blame them.
Still, it seems to me as if that approach merely exchanges the “one size fits all” approach to estrogen with the “no size fits anyone” approach, and is just more of the medical simple-mindedness that pre-dated the WHI. And when has the practice of medicine ever been simple?
The More Measured Response
In a relatively short time, the medical establishment recovered from the acute shock of the WHI. New guidelines for HRT were formulated by the US Preventive Services Task Force, recommending against the use of hormone replacement for the prevention of chronic conditions in women.
But what to do with all those women on HRT for treatment of menopausal symtoms? The WHI did not address these women, and yet they were the ones using most of the HRT. We were essentially left on own to figure this one out. Professional organizations like the American College of Obstetrics and Gynecology and the North American Menopause Society eventually came out with guidelines that were more detailed and helpful than the “just say no” guidelines of the USPSTF. In 2005, the FDA published HRT guidelines for women considering hormonal therapy.
The new guidelines can be summarized simply as: Talk to your doctor, take the lowest dose needed shortest shortest period of time, make sure you know the risks as well as the benefits, and consider alternative treatment when available.
Lower Doses, Shorter Use
The use of HRT for treatment of menopausal symptoms continues to be supported, but at the lowest effective dose for the shortest period of time necessary. Women are now encouraged to try to wean off of estrogen once it is no longer needed for the symptoms of the menopause transition, which last on average about 18 months. For women who continue to need estrogen past that time, the goal is to find the lowest effective dose.
Are lower doses of estrogen safer in terms of heart disease, blood clots, stroke and cancer? No one knows. We do know, however, that they are likely to be just as effective for prevention of osteoporosis, and are often enough to control symptoms. So why take more if less will do?
Vaginal Estrogen
Vaginal estrogen remains a viable option for the many women whose only real symptom is vaginal dryness. To date, I know of no adverse data associated with vaginal estrogen use, except that if the cream is used, one may occasionally get endometrial stimulation. Some experts still recommend some progesterone to balance that out. Newer vaginal estrogen formulations such as the ring or vaginal tablet appear to be quite safe for the endometrium. For women who are concerned, drawing blood levels can confirm that the absence of significant systemic absorption. Additionally, the endometrium can be sonogramed periodically.
Transdermal Estrogen
Since the WHI, some doctors have begun to preferentially prescribe transdermal estrogen, there being some data that it may impact clotting factors less than oral estrogen. Transdermal patches are a good option for women who want to stay with the so-called “bio-identical” estrogen, 17-beta estradiol. Taken orally, this molecule can have a shorter half life, and I have had more than a few patients need to take either higher doses of more frequent dosing to alleviate their hot flashes. For some women, however, patches can irritate the skin, so they are better off with oral.
Progesterone
Natural progesterone has become de rigeuer, although there are no really good data that it is any safer than Provera was. I do prescribe natural progesterone preferentially, because I find it is generally better tolerated than Provera. But I have no major objections to the so-called synthetic progestins, because natural progesterone can make some women very sleepy, even at low doses. (For most this is an advantage, insomnia being a symptom of menopause.)
Transdermal progesterone, while a very popular health food store item, is very variably absorbed through the skin, and not yet available in any reliable product for endometrial protection. As a result, it is not recommended to “balance” the estrogen part of HRT.
Some women cannot tolerate any progestin, oral, transdermal, natural or synthetic. The Mirena IUD might be an option for these women.
Non-Hormonal Options
For symptomatic women unwilling or unable to take HRT, newer non-hormonal options are being studied and offered off-label for treatment of hot flashes. The SSRI’s fluoxetine, paroxetine, venlafaxine and the anti-seizure medication gabapentin have been shown in small controlled trials to reduce hot flashes by about 65%. Not as good as estrogen, but for some women, enough. No large long term trials of these drugs have as yet been done.
Do you see what is happening? We are beginning to custom tailor the therapy to the patient – her needs, her symptoms, her concerns, her side effects. And her risks. Because, most importantly, doctors have began to weigh the risks and benefits of estrogen a little more carefully, patient by patient.
No more one size fits all. And that’s just better medicine, if you ask me.
The Plot Thickens…
Since 2002, the plot has taken a few twists. The first was the publication of data from the estrogen-only arm of the WHI. In that group, breast cancers were actually fewer in women who took Premarin alone, though not statistically so. (Of course, this data got much less attentionia atention than the combined hormone arm of the study.)
This difference between the data on estrogen-alone and combination HRT has led many to believe the the evil hormone is not estrogen, but progesterone. Or more specifically, medroxyprogesterone acetate, the progestin compound in Prempro. But is the so-called “natural” progesterone safer than Provera? Your guess is as good as mine. Again, no long term data.
The second twist has been an analysis of the younger women in the estogen-only arm of the WHI, those who began the drug in their 50’s, in a manner more typical to the way we gynecologists tend to prescribe it. In this group, there was not an increase in heart disease, but a suggestion of a decrease. This would support the hypothesis of a so-called “window of opportunity”, a period of as yet undefined time after menopause during which HRT, if started, might actually do all the heart-friendly things we all had thought it would do.
Recent findings from the Nurse’s Health Study also support this hypothesis, and suggest that for women who use HRT beginning at menopause, the risks of heart disease are reduced almost a third. A randomized, placebo-controlled trial to investigate this possibility is in the works, but don’t expect an answer anytime soon.
The relatively more favorable data from the estrogen-only arm has led science-saavy women to begin to ask for hormone regimens that use less progesterone. The problem with this approach is the ever-present risk of endometrial cancer from long term use of unopposed estrogen. I have some concerns about this – essentially treading off one low cancer risk (breast) for a higher one (uterine). Quarterly progesterone regimens are associated with higher rates of endometrial hyperplasia, and that has been my experience when my patients have tried these regimens. I have had better success with quarterly progestin regimens when they are combined with less than standard doses of estrogen. I have had one patient go to hysterectomy because she kept developing hyperplasia and was no longer willing to take progesterone of any kind, ever.
So, where are we now?
And so, four years later, we are practically back where we started. Maybe estrogen is good for the heart, as long as you start it early enough. Maybe the breast cancer risk isn’t from estrogen, but from progesterone. Maybe lower doses or transdermal regimens will prove to be safer. Maybe, maybe…
So how does a woman make a decision about HRT given all the unanswered questions? Her hot flashes will not wait for a better study to come along. And how does one practice medicine in this era of uncertainty? It’s not easy, I can tell you. You need to be clear in the face of fuzzy data. You must be internally consistent when externally, all is not. You have to be flexible, but not wishy-washy. It isn’t easy, but it can be done.
Up next…How I do it
Category: Second Opinions

 A Few Words About Bioidentical Hormones
A Few Words About Bioidentical Hormones And speaking of hype…
And speaking of hype…















 Over the past 12 years, I’ve gotten my office to run like a well-oiled machine, operated by a top notch office staff and fueled by the various office systems I developed myself. These included a tickler system for lab and radiology results, a patient chart organized so that I could retrieve whatever information I needed in an instant, patient information sheets I’d written myself, and, if you’ve been reading this blog for awhile, you already know about
Over the past 12 years, I’ve gotten my office to run like a well-oiled machine, operated by a top notch office staff and fueled by the various office systems I developed myself. These included a tickler system for lab and radiology results, a patient chart organized so that I could retrieve whatever information I needed in an instant, patient information sheets I’d written myself, and, if you’ve been reading this blog for awhile, you already know about 



 POST-SECOND AVE DELI MUSHROOM BARLEY SOUP
POST-SECOND AVE DELI MUSHROOM BARLEY SOUP






 Raising organic animals is no easy undertaking, and the Gerlachs have had to make some tough choices in the process. When their goats acquired a parasitic infection, they removed them from food-producing because the treatment involved chemical antibiotic use. Did I say that Barbara and Charles are committed?
Raising organic animals is no easy undertaking, and the Gerlachs have had to make some tough choices in the process. When their goats acquired a parasitic infection, they removed them from food-producing because the treatment involved chemical antibiotic use. Did I say that Barbara and Charles are committed?



 What I like best about Berry Fields is that it is so real. This is no Martha Stewart farmette, and while its owners may speak the langauge of the gentleman (and woman) farmer, they are anything but. No pretty clapboard county house, no picturesque red barn here. It’s about the food, the animals and the land, not visual appeal.
What I like best about Berry Fields is that it is so real. This is no Martha Stewart farmette, and while its owners may speak the langauge of the gentleman (and woman) farmer, they are anything but. No pretty clapboard county house, no picturesque red barn here. It’s about the food, the animals and the land, not visual appeal.
{kind=link}
{kind=link}
{kind=link}
{kind=link}